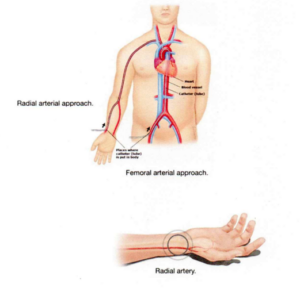
Conventionally an angiography is done via the femoral route. It involves an access gained via femoral artery in the groin. The advantages of this approach is that it is easy to perform and large bore catheters can be used in these interventions. The disadvantages of femoral approach are for the patient. The patient has to lie down, immobilise the limb for five hours after the procedure and there is a 2% to 3% risk of local bleeding complications at the site where the puncture was done. Femoral approach is still regarded as best for Cardiogenic shock management by PCI and introduction of intraaortic balloon counterpulsation and in treatment of chronic total occlusion. Radial approach for coronary angiography and angioplasty is fast gaining acceptance amongst the interventional cardiologists of today. The greatest advantage is the practical absence of bleeding complication in this approach both for angiography and angioplasty. When you cross the learning curve for the radial approach the procedure time required is similar to that for femoral approach and the patient can be mobilised earlier than femoral approach. The sheath which is introduced into the radial artery is immediately removed after the completion of the angioplasty while it takes three hours of time until you wait for the femoral arterial sheath to be removed. Thus the patient has to wait for a total of eight hours after an angioplasty. Once the radial access is gained the next hurdle is canulating the coronary arteries. Once this is done the next approach for coronary angiography or angioplasty is similar to femoral approach.